| Name | Sulphadiazine + Trimethoprim |
| Classes |
Antiinfective Agent Antibiotic Antibiotic Combination |
| Diseases |
Bronchitis Ear Infection Infectious Disease Pneumonia Shigellosis Traveler's Diarrhea UTI (Urinary Tract Infection) |
 Bangla
Bangla English
EnglishSulphadiazine + Trimethoprim
Sulphadiazine + Trimethoprim is a combination of two antimicrobial drugs. Sulfamethoxazole inhibits bacterial synthesis of dihydrofolic acid by competing with para-aminobenzoic acid (PABA). Trimethoprim inhibits the production of tetrahydrofolic acid from dihydrofolic acid by binding to and reversibly inhibiting the required enzyme, dihydrofolate reductase. Thus, sulfamethoxazole and trimethoprim inhibit two consecutive steps in the biosynthesis of nucleic acids and proteins, both of which are required by many bacteria.
Sulphadiazine + Trimethoprim is indicated in the following conditions-
- Pneumocystis Jiroveci Pneumonia
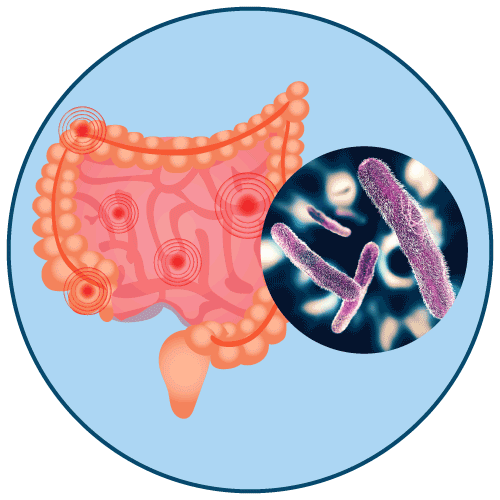
- Shigellosis
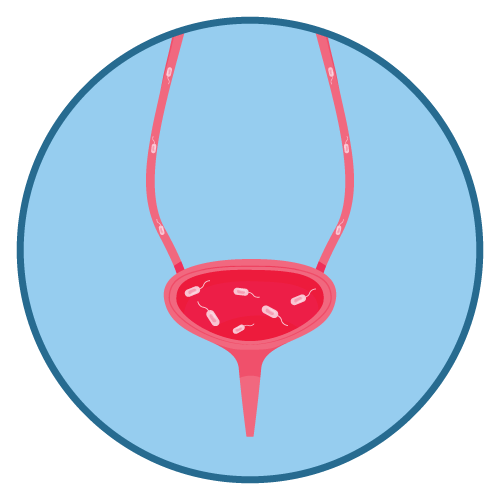
- Urinary Tract Infections
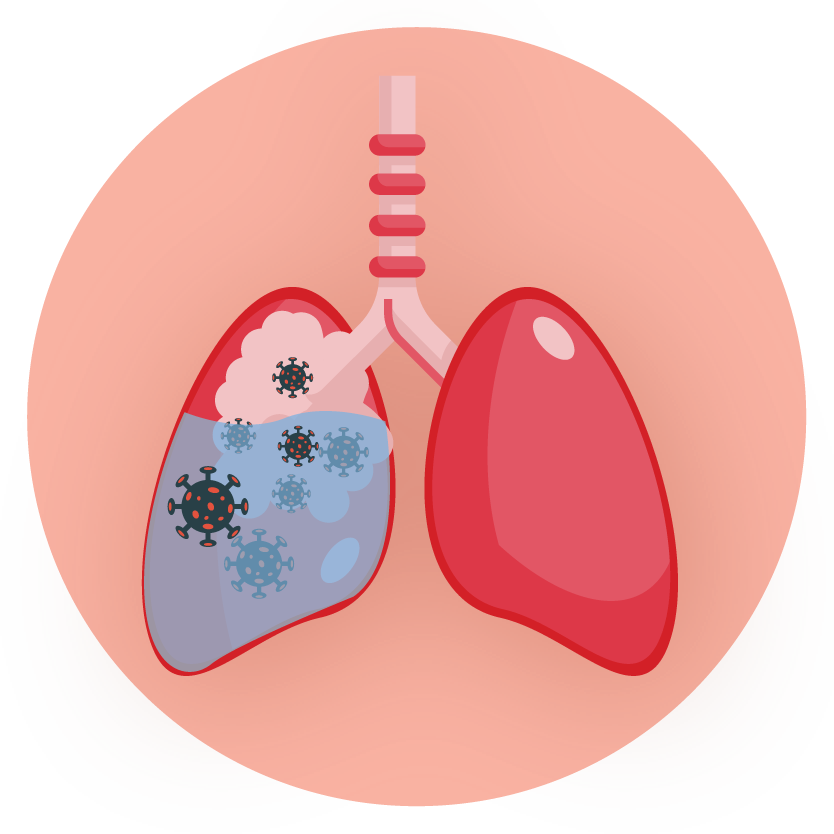
Pneumocystis Jiroveci Pneumonia: Total daily dose is 15 to 20 mg/kg (based on the trimethoprim component) given in 3 or 4 equally divided doses every 6 to 8 hours for up to 14 days. One investigator noted that a total daily dose of 10 to 15 mg/kg was sufficient in 10 adult patients with normal renal function.
Severe Urinary Tract Infections and Shigellosis: Total daily dose is 8 to 10 mg/kg (based on the trimethoprim component) given in 2 or 4 equally divided doses every 6, 8 or 12 hours for up to 14 days for severe urinary tract infections and 5 days for shigellosis. The maximum recommended daily dose is 60 mL per day.
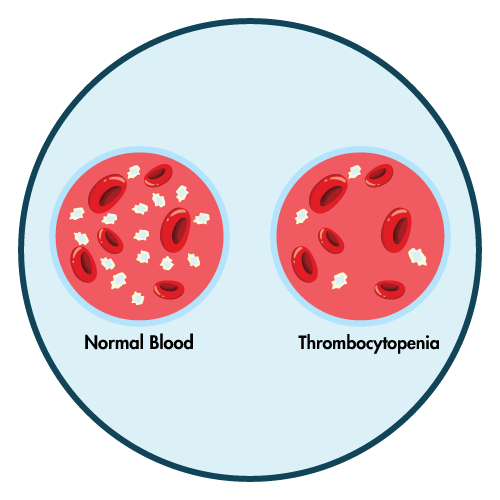
- Hematologic: Agranulocytosis, aplastic anemia, thrombocytopenia, leukopenia, neutropenia, hemolytic anemia, megaloblastic anemia, hypoprothrombinemia, methemoglobinemia, eosinophilia.
- Allergic Reactions: Stevens-Johnson syndrome, toxic epidermal necrolysis, anaphylaxis, allergic myocarditis, erythema multiforme, exfoliative dermatitis, angioedema, drug fever, chills, Henoch-Schoenlein purpura, serum sickness-like syndrome, generalized allergic reactions, generalized skin eruptions, conjunctival and scleral injection, photosensitivity, pruritus, urticaria and rash. In addition, periarteritis nodosa and systemic lupus erythematosus have been reported.
- Gastrointestinal: Hepatitis (including cholestatic jaundice and hepatic necrosis), elevation of serum transaminase and bilirubin, pseudomembranous enterocolitis, pancreatitis, stomatitis, glossitis, nausea, emesis, abdominal pain, diarrhea, anorexia.
- Genitourinary: Renal failure, interstitial nephritis, BUN and serum creatinine elevation, toxic nephrosis with oliguria and anuria, and crystalluria.



Hypersensitivity and Other Fatal Reactions
- SULFONAMIDE-RELATED FATALITIES, WHILE RARE, HAVE OCCURRED DUE TO SEVERE REACTIONS, INCLUDING STEVENS-JOHNSON SYNDROME, TOXIC EPIDERMAL NECROLYSIS, FULMINANT HEPATIC NECROSIS, AGRANULOCYTOSIS, APLASTIC ANEMIA, AND OTHER BLOOD DYSCRASIAS.
- SULFONAMIDES, INCLUDING SULFONAMIDE-CONTAINING PRODUCTS LIKE SULFAMETHOXAZOLE AND TRIMETHOPRIM INJECTION, SHOULD BE DISCONTINUED IF SKIN RASH OR ANY SIGN OF ADVERSE REACTION APPEARS. A skin rash may be followed by a more severe reaction, such as Stevens-Johnson syndrome, toxic epidermal necrolysis, hepatic necrosis, or serious blood disorders in rare cases (see PRECAUTIONS). Clinical symptoms such as rash, sore throat, fever, arthralgia, pallor, purpura, or jaundice may be early warning signs of severe reactions.
- Cough, shortness of breath, and pulmonary infiltrates are respiratory hypersensitivity reactions that have been reported in association with sulfonamide treatment.
- Thrombocytopenia: The thrombocytopenia caused by sulfamethoxazole and trimethoprim may be an immune-mediated disorder. There have been reports of fatal or life-threatening cases of thrombocytopenia. When sulfamethoxazole and trimethoprim are stopped, thrombocytopenia usually resolves within a week.
- Streptococcal Infections and Rheumatic Fever: The sulfonamides should not be used for the treatment of group A beta-hemolytic streptococcal infections. In an established infection, they will not eradicate the streptococcus and, therefore, will not prevent sequelae such as rheumatic fever.
- Clostridium Difficile Associated Diarrhea: Clostridium difficile associated diarrhea (CDAD) has been reported with use of nearly all antibacterial agents, including sulfamethoxazole and trimethoprim, and may range in severity from mild diarrhea to fatal colitis. Treatment with antibacterial agents alters the normal flora of the colon leading to overgrowth of C. difficile.
Contraindication
Sulfamethoxazole and trimethoprim are contraindicated in patients with a known hypersensitivity to trimethoprim or sulfonamides,
None known.
Sulfamethoxazole and trimethoprim are contraindicated in patients-
- with a history of drug-induced immune thrombocytopenia with use of trimethoprim and/or sulfonamides
- with documented megaloblastic anemia due to folate deficiency.
- pregnant patients and nursing mothers
- pediatric patients less than 2 months of age