| Name | Testosterone Decanoate + Testosterone Isocaproate + Testosterone Phenyl propionate + Testosterone Propionate |
| Classes |
Hormonal Agent Sex Hormone Steroid |
| Diseases |
Hormonal Disorder Testosterone Replacement Therapy Transexual Therapy |
 Bangla
Bangla English
EnglishTestosterone Decanoate + Testosterone Isocaproate + Testosterone Phenyl propionate + Testosterone Propionate
Testosterone Decanoate + Testosterone Isocaproate + Testosterone Phenyl propionate + Testosterone Propionate is combination of different types of testosterone preparations. Testosterone is a male sex hormone produced in the testicles. Testosterone is responsible for normal growth and development of the male sex organs and for maintenance of secondary sex characteristics. These effects include growth and maturation of the prostate, seminal vesicles, penis, and scrotum; development of male hair distribution, such as beard, pubic, chest, and axillary hair; laryngeal enlargement, vocal cord thickening, and alterations in body musculature and fat distribution.
Testosterone Decanoate + Testosterone Isocaproate + Testosterone Phenyl propionate + Testosterone Propionate is available as solution for injection.
The use of testosterone injection as a replacement therapy in males is advised in cases where there are signs of endogenous testosterone insufficiency or absence.
- Primary hypogonadism (congenital or acquired)-testicular failure due to cryptorchidism, bilateral torsion, orchitis, vanishing testis syndrome; or orchidectomy.
- Hypogonadotropic hypogonadism (congenital or acquired)- gonadotropin or LHRH deficiency, or pituitary-hypothalamic injury from tumors, trauma, or radiation.


- Prior to initiating Testosterone Undecanoate, confirm the diagnosis of hypogonadism by ensuring that serum testosterone concentrations have been measured in the morning on at least two separate days and that these concentrations are below the normal range.
- Adults: The usual dose is one injection of 1ml per 3 weeks.
-
Female-to-male transsexuals: Different specialist centres have used doses varying from one injection of 1ml every two weeks to one injection of 1ml every four weeks.
Most common adverse reactions associated with testosterone therapy include-
- polycythemia
- diarrhea
- dyspepsia
- eructation
- peripheral edema
- nausea
- increased hematocrit
- headache
- prostatomegaly
- hypertension
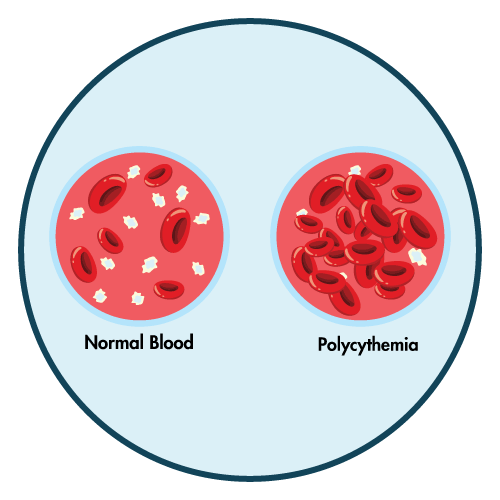
- To identify polycythemia and increasing red blood cell mass, check the hematocrit every three months.
- Patients with benign prostatic hyperplasia (BPH) should be monitored for worsening BPH symptoms and signs.
- Patients using testosterone therapy have been known to experience venous thromboembolism (VTE), including deep vein thrombosis (DVT) and pulmonary embolism (PE). Patients who exhibit symptoms or signs of PE or DVT should be evaluated.
- The most common ways that testosterone has been abused are in combination with other anabolic androgenic drugs and at levels that are greater than those permitted for usage.
- Aazoospermia may result after the administration of androgens exogenously.
- Patients with underlying cardiac, renal, or hepatic illness may experience edema, either with or without congestive heart failure.
- Sleep apnea may occur in those with risk factors.
- Monitor prostate specific antigen (PSA) and lipid concentrations periodically.
- Depression and suicidal ideation have occurred during clinical trials in patients treated with Testosterone therapy.
Contraindication
Contraindicated in patients hypersensitive to testosterone or any of it's ingreients.
None known.
Testosterone Decanoate + Testosterone Isocaproate + Testosterone Phenyl propionate + Testosterone Propionate is contraindicated in-
- Men with breast cancer or known or suspected prostate cancer
- Men with hypogonadal conditions not associated with structural or genetic etiologies
- Pregnancy